Sexual Difference in Effect of Long Sleep Duration on Incident Sarcopenia after Two Years in Community-Dwelling Older Adults
Article information

Abstract
Background
Sarcopenia, a progressive and generalized skeletal muscle disorder involving an accelerated loss of muscle mass and muscle function, is a common condition in older individuals. This study aimed to determine whether sleep latency and duration were independently associated with incident sarcopenia and to explore sex differences in these associations.
Methods
This 2-year longitudinal analysis of cohort study data included community-dwelling participants of the 2016–2017 Korea Frailty and Aging Cohort Study aged 70–84 years at baseline survey who completed the 2-year follow-up survey. Logistic regression was used to calculate the odds ratios (ORs) for sarcopenia and sarcopenia components. Sarcopenia was defined using the 2019 Asian Working Group for Sarcopenia guidelines.
Results
Among 1,353 non-sarcopenic participants in the baseline survey, 1,160 (85.8%) and 193 (14.2%) were classified as non-sarcopenic and sarcopenic, respectively, after 2 years. Long sleep duration (>8 hours per night) was associated with incident sarcopenia in male—OR=2.41 (95% confidence interval [CI], 1.13–5.17) after adjusting for confounding factors. Long sleep duration was specifically associated with the development of low skeletal muscle mass and low muscle strength in male—adjusted OR=2.16 (95% CI, 1.02–4.61) and adjusted OR=2.70 (95% CI, 1.13–6.43), respectively. In female, compared to normal sleep duration, the adjusted ORs for long and short sleep duration for sarcopenia were 2.093 (95% CI, 0.753–5.812; p=0.157) and 0.852 (95% CI, 0.520–1.393; p=0.522), respectively, which were not significant.
Conclusion
In male, long sleep duration was associated with incident sarcopenia, specifically the development of low muscle mass and low muscle strength, but not with low physical performance.
INTRODUCTION
Aging is frequently accompanied by changes in sleep patterns, including increased sleep disturbances, which affect up to 50% of the population.1) Sleep disturbances are associated with increased risks of coronary disease, hypertension, diabetes, and mortality.2-5) Marked changes in sleep structure with aging have been reported, including decreased total sleep time and sleep efficiency and increased wake time after sleep onset.6)
Sarcopenia, a progressive and generalized skeletal muscle disorder involving an accelerated loss of muscle mass and muscle function, is a common condition in older individuals.7) The prevalence of sarcopenia ranges from 4% to 46.8% according to different diagnostic criteria.8) Sarcopenia contributes significantly to morbidity, decreased quality of life, and increased health care costs in older adults.9) In particular, sarcopenia is significantly correlated with cardiometabolic risk factors, especially diabetes, hypertension, and dyslipidemia.10)
Several studies have indicated a relationship between sleep disturbances and sarcopenia.11-13) Kwon et al.12) showed that long sleep duration (≥9 hours) was independently associated with sarcopenia in Korean adults, while Hu et al.13) showed a U-shaped relationship between self-reported sleep duration and sarcopenia in Chinese community-dwelling older female. These previous studies were cross-sectional, a study design that did not allow the inference of causality between sleep disturbance and sarcopenia.11-13) Recently, in a 4-year longitudinal study, Nakakubo et al.14) showed an association between long sleep duration and the risk of progression to sarcopenia among older Japanese adults. However, this study did not explore the effect of sleep latency or sex differences on these associations. Related studies have reported conflicting findings regarding sex differences, which may be attributed to different daily sleep duration and/or requirements between sexes due to their different hormone levels.15) Sex hormones also regulate muscle mass and function and differ between sexes.16) Therefore, this study aimed to determine whether sleep latency and duration were independently associated with incident sarcopenia in community-dwelling older adults and to explore the sex differences in these associations.
MATERIALS AND METHODS
Participants
This study involved participants of the Korean Frailty and Aging Cohort Study (KFACS).17) The KFACS is a national, multi-center, longitudinal cohort study. The baseline survey was conducted from 2016 to 2017, with a target number of 3,000 adults aged 70–84 years. The participants were recruited from 10 medical centers (8 hospitals and 2 public health centers) nationwide. For the 3,014 baseline survey participants, the first follow-up surveys (n=2,864) were conducted from 2018 to 2019. Participants with missing data were excluded. The analysis in the present study included participants who did not have sarcopenia at baseline and who participated in the follow-up survey 2 years later (n=1,353).
Sleep Parameters
Sleep parameters were reported by the participants using a questionnaire about their usual sleep patterns for the past 4 weeks. Two questions about subjective sleep quality were extracted from the Pittsburgh Sleep Quality Index (PSQI) questionnaire: (1) How long (in minutes) has it taken you to fall asleep each night? (2) How many hours of actual sleep did you get at night?18) The sleep latency and sleep duration measures were based on the answers provided. A previous meta-analysis reported that sleep duration and the relative risk of sarcopenia showed a nonlinear U-shaped association, with nadirs at 6 hours and 8 hours of sleep per day.19) Based on these findings, we categorized sleep duration as short (<6 hours), average (6–8 hours), or long (>8 hours). We defined prolonged sleep latency as taking more than 60 minutes to fall asleep.20)
Definition of Sarcopenia
Sarcopenia was defined according to the 2019 Asian Working Group for Sarcopenia (AWGS) guidelines as low muscle mass plus low muscle strength or low physical performance.
The AWGS 2019 cutoffs for low muscle mass for sarcopenia diagnosis are height-adjusted appendicular skeletal muscle (ASM) <7.0 kg/m2 in male and <5.4 kg/m2 in female. Height-adjusted ASM was defined as ASM (kg)/height (m2), as measured using dual-energy X-ray absorptiometry (DXA)—Lunar (GE Healthcare, Madison, WI, USA) and Hologic DXA (Hologic Inc., Bedford, MA, USA). ASM was calculated as the sum of the lean mass of the right and left arms and legs under the assumption that all non-fat and non-bone tissues were skeletal muscles. Handgrip strength, measured using a digital handgrip dynamometer (T.K.K.5401; Takei Scientific Instruments Co. Ltd., Tokyo, Japan), was used to indicate low muscle strength. The diagnostic cutoffs for handgrip strength were <28.0 kg for male and <18.0 kg for female. The participants were instructed to squeeze the handle with maximum effort for 3 seconds using each hand. Each hand was tested twice, and maximum handgrip strength was defined as the highest measurement for each hand, expressed in kilograms. Physical performance was evaluated using the usual gait speed, five-times sit-to-stand test, and the Short Physical Performance Battery (SPPB). The cutoff for low physical performance was usual gait speed <1 m/s, five-time chair stand time ≥12 seconds, or SPPB score ≤9. Low physical performance was defined as obtaining values below the cutoff for any one of these three tests. The usual gait speed over a distance of 4 m was measured using an automatic gait speed meter (Dynamicphysiology, Daejeon, Korea) with acceleration and deceleration phases of 1.5 m each. The participants were asked to perform the test by walking at a normal pace. The five-times sit-to-stand test measures the time required to stand five times from a sitting position without using the arms from a straight-backed armchair as quickly as possible. The SPPB consists of three standing-balance measures, five chair-stand time measures, and an assessment of usual gait speed. Each test was assigned a score of 0–4, based on the normative scores obtained from the Established Population for Epidemiologic Studies of the Elderly, with a total score ranging from 0 to 12.21,22)
Other Variables
The medical histories of participants were noted from a predefined list of chronic health conditions. Low physical activity levels were defined as <494.65 kcal/week for male and <283.50 kcal/week for female, corresponding to the lowest 20% of the total energy consumed in a population-based Korean survey of older adults from among the general population.17) Energy expenditure estimates (kcal/week) were calculated using the International Physical Activity Questionnaire (IPAQ), and metabolic equivalent scores were derived according to vigorous, moderate, and mild activity responses in the questionnaire. Nutritional status was rated using the Korean version of the Short Form of the Mini-Nutritional Assessment (MNA), and participants who scored ≤11 or less were considered as at risk for malnutrition or with malnutrition.23) A 15-item Korean version of the Short Form Geriatric Depression Scale (GDS-K) was used to evaluate depression, with scores ≥6 defined as suggestive of depression.24) Polypharmacy was defined as the use of five or more prescribed medicines for >3 months. Muscle quality of the arms (MQIArm, kg/kg) was defined as the ratio between the dominant handgrip strength and dominant arm ASM.25) We defined low MQIArm as -1 SD in our study population, which was 11.04 in male and 10.03 in female.26)
Ethical Approval
The present study was submitted to and exempt from the requirement for Institutional Review Board approval by the Clinical Research Ethics Committee of Kyung Hee University Medical Center (IRB No. 2021-03-057) and complied with the ethical rules for human experimentation described in the Declaration of Helsinki. Informed consent was obtained from all participants or their proxy.
Also this study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.27)
Statistical Analysis
We compared characteristics according to sarcopenia category using independent-sample t-tests and chi-square tests for continuous and categorical data, respectively. After univariate analysis, we included factors with p<0.1 as adjustment factors in multivariate logistic regression analyses. Statistical analysis was performed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA), and significance was defined as a p-value <0.05.
RESULTS
General Characteristics of the Study Population
Among 1,353 non-sarcopenic participants at baseline, 1,160 (85.7%) were classified as non-sarcopenic and 193 (14.3%) as sarcopenic 2 years later, according to the 2019 AWGS guidelines (Table 1). The median ages of the non-sarcopenic and sarcopenic participants were 75.3 and 76.4 years in male and 74.9 and 76.4 years in female, respectively. The prevalence of cerebrovascular disease (CVD), angina, and depression was higher in men in the sarcopenic group than that in those in the non-sarcopenic group. The prevalence of CVD was higher than male in female with sarcopenia. The rates of low physical activity in non-sarcopenic and sarcopenic participants were 4.5% and 12.6% in male and 7.0% and 16.7% in female, respectively. The median sleep duration was 6.4 hours in both non-sarcopenic and sarcopenic male and 5.9 and 6.0 hours in non-sarcopenic and sarcopenic female, respectively. The rates of long sleep duration (total sleep time >8 hours per night) in non-sarcopenic and sarcopenic participants were 5.7% and 11.7% in male and 3.5% and 6.7% in female, respectively (Table 1).
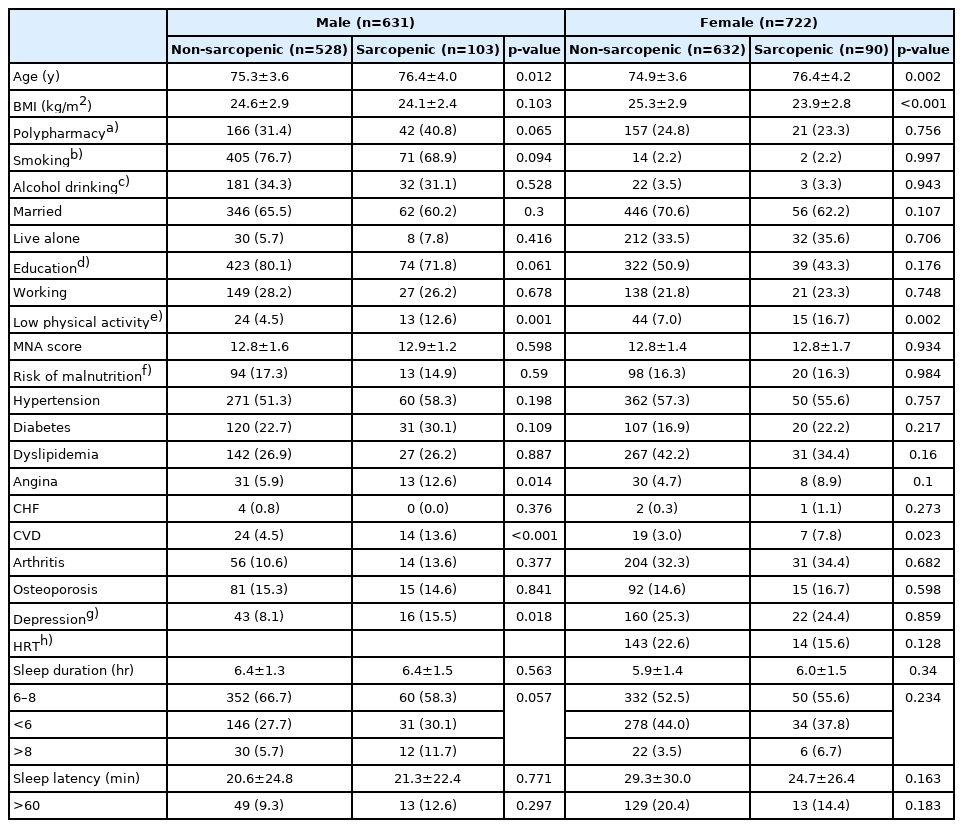
Characteristics of study participants, according to sarcopenia status at 2 years
Sleep Patterns and Incident Sarcopenia in Male
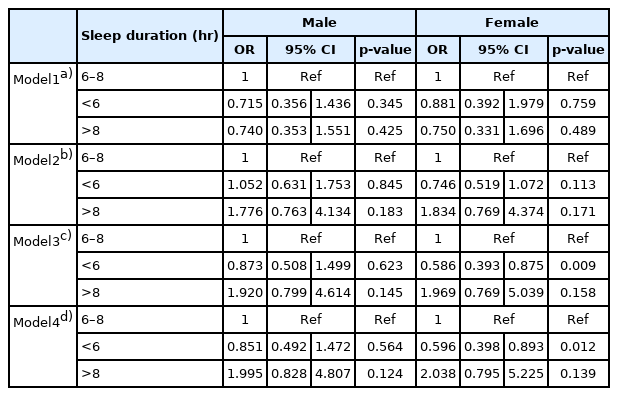
Long sleep duration (>8 hours) in male was associated with greater odds of incident sarcopenia after 2 years compared to the reference (6–8 hours). After adjusting for multiple factors including age, body mass index (BMI), smoking, polypharmacy, education, angina, CVD, depression, and physical activity, the association between long sleep duration and incident sarcopenia remained significant (odds ratio [OR]=2.410; 95% confidence interval [CI], 1.125–5.166; p=0.024). In comparison, short sleep duration (<6 hours) was not associated with sarcopenia development in male (OR=1.192; 95% CI, 0.725–1.960; p=0.488). Prolonged sleep latency (≥60 minutes) was not associated with sarcopenia in male (OR=1.014; 95% CI, 0.505–2.036; p=0.969) (Tables 2, 3).

Odds ratio of sleep duration relationship to incident sarcopenia, by sex
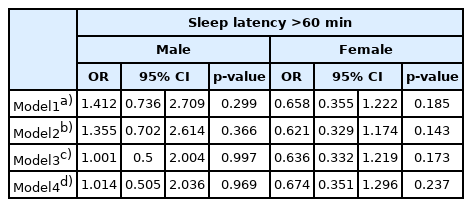
Odds ratio of sleep latency relationship to incident sarcopenia, by sex
Sleep Patterns and Incident Sarcopenia in Female
Compared to normal sleep duration, the adjusted ORs for long and short sleep duration for sarcopenic female were 2.093 (95% CI, 0.753–5.812; p=0.157) and 0.852 (95% CI, 0.520–1.393; p=0.522), respectively, which were not significant. Prolonged sleep latency (≥60 minutes) was not associated with sarcopenia in female (OR=0.674; 95% CI, 0.351–1.296; p=0.237) (Tables 2, 3).
Effects of Sleep Duration on Sarcopenia Components in male
In male, after adjusting for multiple factors (including age, BMI, polypharmacy, alcohol, education, employment status, hypertension, osteoporosis, and depression), the association between long sleep duration and low muscle mass was significant (OR=2.163; 95% CI, 1.016–4.605; p=0.045) (Table 4). The association between long sleep duration and low muscle strength remained significant after adjusting for multiple correlates (OR=2.695; 95% CI, 1.130–6.431; p=0.025) (Table 5). However, long sleep duration was not associated with low physical performance (OR=1.075; 95% CI, 0.546–2.117; p=0.833) in male (Table 6). Short sleep duration (<6 hours) was not associated with any sarcopenia component (low muscle mass, low muscle strength, or low physical performance) in unadjusted or adjusted analyses (Tables 4–6). Sleep duration was not associated with muscle quality after adjusting for multiple factors (Supplementary Table S2).

Odds ratio of sleep duration relationship to low height-adjusted ASM index, 2-year follow-up, by sex

Odds ratio of sleep duration relationship to low muscle strength, 2-year follow-up, by sex

Odds ratio of sleep duration relationship to low physical performance, 2-year follow-up, by sex
Effects of Sleep Duration on Sarcopenia Components in Female
In female, after adjusting for multiple factors, the ORs of long sleep duration for low height-adjusted ASM, low muscle strength, and low physical performance were 0.766 (95% CI, 0.278–2.105; p=0.605), 1.997 (95% CI, 0.884–4.511; p=0.096), and 1.885 (95% CI, 0.879–4.042; p=0.103) (Tables 4–6, respectively). Short sleep duration (<6 hours) was not associated with any sarcopenia component (low muscle mass, low muscle strength, or low physical performance) in the adjusted analyses. However, low gait speed and low SPPB score showed associations with short sleep duration (Tables 7, 8). Long 5 sit-to-stand test didn’t showed association with sleep duration (Table 9).
Odds ratio of sleep duration relationship to low gait speed, 2-year follow-up, by sex

Odds ratio of sleep duration relationship to low SPPB test, 2-year follow-up, by sex

Odds ratio of sleep duration relationship to long 5 sit-to-stand test, 2-year follow-up, by sex
DISCUSSION
The results of our study in community-dwelling older adults showed that long sleep duration, compared with normal sleep duration, increased the risk of incident sarcopenia after 2 years in male. Regarding sarcopenia components, long sleep duration was associated with low muscle mass and strength after 2 years in male.
Chronic inflammation and insulin resistance, and brain pituitary function are all important mechanisms explaining the relationship between long sleep duration and sarcopenia. Long sleep duration is also closely associated with increased insulin resistance.28) Insulin resistance contributes to decreased synthesis of skeletal mass protein, leading to sarcopenia in older adults.29) Another mechanism for the relationship between sleep duration and sarcopenia could be chronic inflammation. Long-duration sleepers have significantly higher levels of proinflammatory markers, such as C-reactive protein and interleukin-6 (IL-6),30) and inflammatory mediators play an important role in the development of sarcopenia by promoting muscle proteolysis. The results of a population-based study demonstrated significantly elevated circulating concentrations of IL-6 and tumor necrosis factor-α (TNF-α) in older adults with sarcopenia and showed that higher IL-6 and C-reactive protein (CRP) levels increased the risk of muscle strength loss.31) Chronic inflammation might affect the anabolic and catabolic metabolism of muscles, resulting in sarcopenia.30) The results of a recent meta-analysis revealed that higher IL-6 and CRP levels were significantly associated with long but not short sleep duration.32) In addition, disrupted circadian rhythm, which is controlled by the brain, and hormonal changes associated with long sleep durations might also be a possible underlying mechanism explaining the link between long sleep duration and sarcopenia.33) These findings might explain the association between long sleep duration and incident sarcopenia. In our study, CRP level was not associated with incident sarcopenia; however, insulin resistance showed an association in male (Supplementary Table S1), which may explain some of the association between long sleep duration and incident sarcopenia in male.
In female, short sleep duration was positively associated with low physical performance such as slow gait speed (OR=0.564) and poor SPPB score (OR=0.656). Older age is more strongly associated with poor subjectively reported sleep in female, and older female consistently report shorter and poorer sleep compared to older male.34) However, actigraphic sleep measures showed poorer sleep in male.35,36) The results of the Health ABC cohort study showed that thigh muscle mass was not associated with gait speed changes in female. However, all fat composition variables were associated with gait speed decline after 4 years.37) Furthermore, female are generally at a higher risk of osteoarthritis incidence and disease severity than male.38) These factors might explain the association of short sleep duration with slow gait speed and poor SPPB score. However, low physical performance was not associated with short sleep duration in female.
Sleep latency was not a significant predictor of sarcopenia in our study. In the previous two related publications, one study reported higher scores for sleep latency in sarcopenic subjects compared with those in non-sarcopenic subjects (p=0.03) after adjusting for confounders39); however, the other study did not find that sleep latency was associated with sarcopenia in middle-aged individuals.40) Yet another study20) postulated that depression was an intermediating factor between long sleep latency and frailty in older Korean male; therefore, sleep latency was not directly associated with frailty. However, these papers were cross-sectional designs; therefore, the results of our prospective study demonstrate the cause-effect relationship.
To our knowledge, no other longitudinal study has reported the sex-specific effects of sleep duration on incident sarcopenia in older adults. Nakakubo et al.14) reported that long sleep duration was associated with an increased risk of progression to sarcopenia among older adults but did not show differences in the association according to sex. However, they did report that long sleep duration was associated with slow gait and lower grip strength but not with lower muscle mass, contrary to our findings. To evaluate ASM, Nakakubo et al.14) used multi-frequency bioelectrical impedance analysis, which can overestimate ASM compared to DXA,41) which could explain the divergent results. Additionally, unlike the association of long sleep duration with slow gait and low grip strength after 4 years reported by Nakakubo et al.,14) we observed a relationship between sleep duration and muscle mass and strength but not physical performance in male only. However, 2 years may have been too short a duration to observe decreased physical performance.
In this study, we observed sex differences in the association between long sleep duration and incident sarcopenia. Unlike previous cross-sectional studies that reported the association of sleep duration with sarcopenia in female 13) and both sexes,19) we observed an association only in male. However, both previous studies were cross-sectional and only two studies have reported on the longitudinal effect of long sleep duration on sarcopenia,14,42) neither of which investigated sex differences in this relationship. Therefore, our findings demonstrate the difference in the cause-effect relationships of long sleep duration on incident sarcopenia. We observed this relationship only in male; thus, the relationship reported in female in cross-sectional studies may have been coincidental findings. The sex difference in the effects of long sleep duration on sarcopenia may occur due to the different requirements for sleep duration between the sexes owing to their different hormone levels.15) Furthermore, female are more resilient to environmental stressors. Another explanation for the differential association according to sex may be that muscle mass declines more slowly in female than in male. A previous study reported a steeper decline in relative skeletal muscle mass (kg/m2) in male (15.2 − 0.07 × age; p<0.001) compared with that in female (8.9 − 0.02 × age; p<0.001).43) Therefore, a 2-year follow-up may have been insufficient to determine the effect of sleep duration on incident sarcopenia in female.
This study had several limitations. First, the sleep variables were based on participant recall, which may lead to bias and differ from objective sleep measurements. One study reported that self-reported sleep latency was 10 minutes longer than objectively measured sleep latency and that the estimated total sleep duration was slightly shorter than the measured duration (median difference, -18.5 minutes) in adults with a mean age of 50 years.20,44) Second, as the participants of this study were community-dwelling older adults, the results do not represent the entire population of older Korean adults as we did not include hospitalized, institutionalized, or bedridden older adults.
The study also has several strengths. We enrolled a relatively large number of community-dwelling older adults aged 70–84 years, and the cohort was gathered from 10 regions nationwide, including urban and rural areas of Korea. Therefore, the cohort was representative of the community-living age group across Korea. Previous studies have reported controversial associations between sleep duration and sarcopenia; however, no other studies have investigated sex differences in the effect of long sleep duration on incident sarcopenia. We observed that long sleep duration (>8 hours per night) was associated with high odds for incident sarcopenia after 2 years in male. Interventional studies are needed to investigate if the effect of a reduction in sleep time in these long sleepers can decrease their risk of sarcopenia.
In conclusion, after 2 years of follow-up, long sleep duration (>8 hours per night) was associated with high odds for incident sarcopenia, and the main correlates of incident sarcopenia due to long sleep duration were muscle mass loss and declining muscle strength in male. In contrast, long sleep duration in female was not associated with incident sarcopenia.
Notes
The authors are grateful to the Korean Frailty and Aging Cohort Study Group.
CONFLICT OF INTEREST
The researchers claim no conflicts of interest.
FUNDING
This study was funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HI15C3153). This study was supported by a grant from the Korea Health Technology R&D Project through the Korean Health Industry Development Institute (KHIDI).
AUTHOR CONTRIBUTIONS
Conceptualization, CWW, HL; Data curation, HL, SK; Funding acquisition, CWW; Investigation, CWW, SK; Methodology, CWW, SK, HL; Project administration, CWW; Supervision, CWW; Writing-original draft, HL; Writing-review and editing, HL, SK, BSK, MK, JY, HB, CWW.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4235/agmr.22.0093.
Insulin resistance and inflammation of study participants according to incident sarcopenia, 2-year follow-up, by sex
Odds ratio of sleep duration relationship to index (MQIArm), 2-year follow-up, by sex