



INTRODUCTION
Inadvertent perioperative hypothermia, defined as a decrease in core temperature to <36°C, occurs in 25%–90% of patients undergoing elective surgery.1) Perioperative hypothermia may lead to cardiac morbidity, surgical wound infection, pressure ulcers, deep vein thrombosis, coagulopathy, transfusion, impaired mentation, patient discomfort, prolonged hospitalization, and mortality.2,3) Older patients are particularly vulnerable to perioperative hypothermia due to a loss of subcutaneous fat, a blunted vasoconstrictive response, and decreased heat production.4) The risk of adverse effects also increases with age due to reduced physiological reserves.5)
The primary cause of perioperative hypothermia in patients undergoing surgery under regional or general anesthesia is core-to-peripheral body heat redistribution due to anesthesia-induced vasodilation and central inhibition of thermoregulatory vasoconstriction,2) although the heat loss caused by redistribution is smaller for regional anesthesia compared to general anesthesia.6) Active convective skin warming before anesthesia induction (i.e., prewarming) increases the overall body heat content and reduces the core-to-peripheral tissue temperature gradient. In turn, this reduces the reduction in core temperature due to heat redistribution after anesthesia induction.1)
For hand or upper extremity surgery, regional anesthesia such as brachial plexus block (BPB) can be used instead of general anesthesia. BPB may be preferable to general anesthesia in older patients who are at a greater risk of postoperative morbidity because it is superior in terms of recovery, analgesic consumption, and respiratory complications.7,8) However, there remain no definitive guidelines for the prevention of perioperative hypothermia using interventions such as temperature monitoring and prewarming in patients undergoing surgery using peripheral nerve blocks. The effects of BPB on thermoregulation and the clinical efficacy of prewarming in older patients undergoing BPB have not been established.9) Therefore, this study evaluated the effects of BPB on thermoregulation and the efficacy of prewarming in older patients undergoing hand surgery with BPB by assessing perioperative core temperatures with and without active prewarming using a convective forced-air warmer.
MATERIAL AND METHODS
This prospective, randomized, controlled study was performed between December 2019 and February 2021 at a single university hospital. This study was approved by the Institutional Review Board of Konyang University Hospital (No. 2019-01-004) and registered with the Korea Clinical Research Information Service (https://cris.nih.go.kr/). Written informed consent was obtained from the participants and/or their legal representatives. This study complied the ethical guidelines for authorship and publishing in the Annals of Geriatric Medicine and Research.10)
This study included patients aged ≥65 years undergoing orthopedic hand surgery under BPB and with an American Society of Anesthesiologists physical status of I–III. The exclusion criteria were preoperative core temperature ≥37.5°C or <36.0°C, obesity (body mass index >35 kg/m2), endocrine or metabolic disease (e.g., uncontrolled diabetes, hypothyroidism, etc.), history of alcohol abuse, bleeding tendency, local infection at the BPB injection site, neuropsychiatric disease, or cognitive disorder.
The patients were randomly allocated to either the control or prewarming group (1:1 ratio) using a random number table generated by an online software tool (https://www.randomizer.org). When the patient arrived at the preanesthetic holding area, an anesthesia nurse blinded to the study purpose and not involved in data collection opened a non-translucent envelope containing the patient’s group allocation.
In our institution, the ambient temperatures in the preoperative holding area and post-anesthesia care unit (PACU) were maintained at 22°C–25°C, whereas the ambient operating room temperature was maintained at 21°C–24°C.
All patients arrived at the preanesthetic holding area without premedication and having fasted for a minimum of 8 hours. In the preanesthetic holding area, the control group received standard preoperative passive insulation using a cotton blanket. The prewarming group received 20 minutes of active prewarming using a forced-air blanket (Bair Hugger Full Body Blanket Model 30000; Arizant Healthcare Inc., Eden Prairie, MN, USA) placed over the entire body and then covered with a cotton blanket. During this period, active forced-air warmers were set to 43°C (high) and adjusted to 38°C (medium) if the temperature was too warm for the patient. At the end of active warming, the forced-air blankets were removed, and the patients were covered with cotton blankets and transferred to the operating room.
Patients from both groups received the same anesthetic and surgical management by an anesthesiologist and a surgeon who were blinded to the group assignments. Under ultrasound and nerve stimulator guidance, interscalene BPB was performed using 20–25 mL 0.5% ropivacaine. The time required for interscalene BPB (from needle puncture to needle removal after injection) was recorded. After confirming anesthesia using a pin-prick test, all patients underwent orthopedic hand surgery by the same surgeon. During surgery, the patients were covered with a surgical drape over the cotton blanket, not a forced-air warmer, and received unwarmed fluids. If the patient requested sedation, a small amount (0.5–2 mg) of midazolam was administered intravenously at the anesthesiologist’s discretion. Postoperatively, all patients were transferred to the PACU and covered with a cotton blanket.
We collected data on patient characteristics such as age, sex, weight, height, American Society of Anesthesiologists (ASA) physical status, incidence and amount of administered midazolam, administered fluid, estimated blood loss, duration of anesthesia, and duration of surgery.
Outcome Measurements
The temperature of all patients was measured by a trained anesthesiology resident using an infrared tympanic thermometer (Thermoscan IRT 4020; Braun GmbH, Kronberg, Germany)—accurate to ±0.2°C for temperatures 35.5°C–42°C and to ±0.3°C for temperatures <35.5°C. The highest value of at least two consecutive measurements from the same ear was recorded. The tympanic temperature was measured immediately after arrival in the preanesthetic holding area, on arrival in the operating room, immediately after BPB completion, and at 15-minute intervals during surgery and in the PACU. The tympanic temperature measured immediately after arrival at the preanesthetic holding area was considered the baseline core temperature. Hypothermia was defined as a tympanic temperature ˂36°C. The severity of hypothermia (mild, 35°C–35.9°C; moderate, 34°C–34.9°C; severe, ≤34°C)11) and maximum temperature change (difference between the baseline core temperature and lowest temperature between arrival in the operating room and PACU discharge) were also recorded.
The thermal comfort of the patients was evaluated using a numeric rating scale (0=completely uncomfortable, 10=completely comfortable) immediately after arrival in the preanesthetic holding area (before surgery) and PACU (after surgery).12)
After the BPB procedure and until discharge from the PACU, shivering was evaluated using a 4-point scale (0=no shivering; 1=intermittent, low-intensity shivering; 2=moderate shivering; 3=continuous, intense shivering),13) and the highest value was recorded.
The primary outcome was the core temperature at the end of surgery. The secondary outcomes included maximum temperature change, hypothermia incidence and severity during the perioperative period (i.e., from arrival at the preanesthetic holding area to PACU discharge), perioperative temperature changes, perioperative thermal comfort scores, and perioperative shivering grade.
Statistical Analysis
The smallest difference required to detect hypothermia-related adverse effects is 0.5°C.2,14) A sample size of 16 patients in each group was required to detect a temperature difference of 0.5°C (±0.5°C) at the end of surgery, with a power of 0.8 and a two-sided α-value of 0.05. To compensate for potential dropouts, 20 patients were recruited into each group.
The data distribution of continuous variables was assessed using the Kolmogorov–Smirnov test. Normally distributed variables were analyzed using the Student t-test, while non-normally distributed variables were analyzed using the Mann–Whitney U test. Changes in tympanic membrane temperature over time were assessed using repeated-measures analysis of variance with Bonferroni correction. Categorical variables were analyzed using χ2 tests, χ2 tests for trends (linear-by-linear associations), or Fisher exact tests, as appropriate. Statistical significance was defined as a two-sided p-value of <0.05. Statistical analyses were performed using PASW Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 74 patients were screened and 34 were excluded (11 due to uncontrolled diabetes, eight due to a history of neuropsychiatric disease, four due to a bleeding tendency, three due to cognitive disorders, and eight who refused to participate in the study and preferred surgery under general anesthesia instead of BPB) (Fig. 1). The patient characteristics were comparable between the groups (Table 1).
The temperatures at baseline and on arrival in the operating room did not differ significantly between the groups (Table 2). The primary outcome variable, i.e., the temperature at the end of surgery, did not show a group difference (36.9°C±0.5°C and 37.0°C±0.4°C in the control and prewarming groups, respectively; mean difference=-0.16; 95% confidence interval [CI], -0.44 to 0.12; p=0.252). The maximum temperature change was significantly lower in the prewarming group compared to the control group (0.36°C±0.4°C and 0.65°C±0.3°C, respectively; mean difference=0.29; 95% CI, 0.06 to 0.50; p=0.013). The incidence and severity of perioperative hypothermia did not differ significantly between the groups (p>0.05).
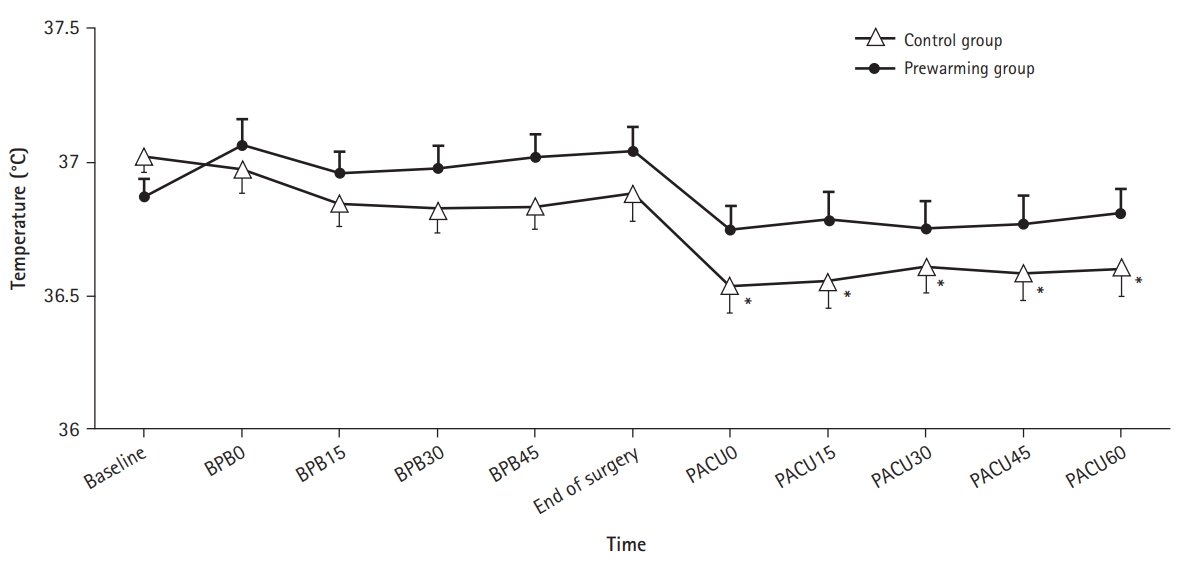
Fig. 2 shows the perioperative changes in tympanic membrane temperature in both groups. In the prewarming group, the tympanic temperature did not differ significantly from baseline during the entire perioperative period. In the control group, the tympanic temperature was significantly lower than the baseline temperature immediately and 15 and 45 minutes after arrival in the PACU (p<0.001), as well as 30 and 60 minutes after arrival (p=0.001). However, the tympanic temperature showed no group differences at any time point (all p>0.05). Perioperative changes in tympanic membrane temperature also did not differ significantly between the groups (p=0.353) (Fig. 2).
The perioperative thermal comfort scores and shivering grades did not differ between the groups (all p >0.05) (Table 2).
DISCUSSION
This study investigated the effects of BPB on the core temperature in older patients who were vulnerable to perioperative hypothermia. We also assessed the efficacy of active prewarming in patients undergoing hand surgery with BPB by comparing the control and prewarming groups. Although the maximum temperature change differed significantly between the two groups, the mean temperature at the end of surgery was close to 37°C regardless of prewarming, with no significant difference from the baseline temperatures observed in either group. In addition, although perioperative hypothermia occurred in 10% (2/20) and 5% (1/20) of patients in the control and prewarming groups, respectively, its severity was mild in all cases. This suggests that unlike general or neuraxial anesthesia, peripheral nerve blocks, such as BPB, do not significantly affect thermoregulatory function, even in older patients. Thus, the clinical effect of active prewarming in older patients undergoing hand surgery with BPB did not appear to be significant.
Previous studies have suggested that core temperature monitoring may be unnecessary in patients undergoing surgery under peripheral nerve block because the effects of peripheral nerve block are restricted to local thermoregulatory responses.14) However, to our knowledge, no prospective randomized controlled trials have been conducted to validate this suggestion. Moreover, advanced age is a well-known risk factor for hypothermia under both general and regional anesthesia1,15,16) and, in the case of regional anesthesia, the core temperature of adult patients may decrease by 0.03°C with increasing age.16) Furthermore, although preventive interventions for inadvertent hypothermia are recommended for procedures exceeding 30 minutes in duration,17) the efficacy of prewarming in patients undergoing surgery under BPB remains uncertain.9) The results of the present study may shed light on these unresolved issues.
A retrospective cohort study of adult patients undergoing orthopedic surgery under BPB reported an incidence of postoperative hypothermia of 40.6%.9) Moreover, a lower preoperative core temperature, history of alcohol abuse, arthroscopic shoulder surgery, use of fentanyl, concomitant use of sedatives, larger amounts of intravenous fluids, and longer duration of surgery were predictors of postoperative hypothermia.9) Based on these results, the authors recommended temperature monitoring as a standard of care in patients undergoing surgery under BPB. However, the effects of BPB on thermoregulation could not be assessed because factors that could affect the incidence of hypothermia, such as underlying diseases (e.g., hypothyroidism, alcohol abuse), surgery type (e.g., arthroscopic shoulder surgery requiring large volumes of irrigation solution), analgesic use (e.g., fentanyl, morphine, pethidine), and sedative use (e.g., midazolam, propofol, dexmedetomidine) were not controlled. Additionally, prewarming was not performed in all patients; therefore, whether prewarming contributed to the prevention of hypothermia could not be assessed. Our study excluded patients with a history of diseases that could affect thermoregulation and the type of surgery was limited to non-arthroscopic orthopedic hand surgery. Additionally, no intraoperative analgesics were administered and only midazolam was used as an intraoperative sedative, which does not noticeably impair thermoregulation.18)
In this study, the mean tympanic temperatures at the end of surgery were 36.9°C and 37°C, and the incidence of perioperative hypothermia was 10% and 5%, in the control and prewarming groups, respectively. A retrospective study of older patients undergoing arthroscopic shoulder surgery under BPB with propofol sedation19) reported an incidence of perioperative hypothermia of 9.2%, which was comparable to the control group in our study. In another retrospective study of older patients who underwent both BPB and general anesthesia,20) the mean tympanic temperature on PACU arrival was 35.3°C, and 93.1% of the patients were hypothermic. Similarly, in a prospective study of 50–80-year-old patients undergoing spinal anesthesia, the tympanic temperature on arrival at the PACU was 35.6°C, and 88% of the patients showed hypothermia.21) Unwarmed patients undergoing general or neuraxial anesthesia reportedly experience a decrease in core temperature of approximately 1°C–2°C.14) In patients under general anesthesia, the core temperature decreased by 1.6°C±0.3°C during the first hour after induction of anesthesia.22) Meanwhile, spinal anesthesia decreased the core temperature by 1.0°C±0.3°C during the perioperative period.12) In the present study, the maximum temperature changes during the perioperative period were 0.36°C±0.3°C and 0.65°C±0.3°C in the prewarming and control groups, respectively. Thus, regardless of prewarming, BPB caused less core temperature reduction than general or neuraxial anesthesia. The extent of impairment of thermoregulatory control in patients undergoing surgery under regional anesthesia is proportional to the level of blockade.16) Therefore, BPB, which causes nerve block in only one upper extremity, did not significantly affect thermoregulation compared to neuraxial anesthesia.
Prewarming is the best way to prevent hypothermia caused by the redistribution of body heat following anesthesia.23) Among prewarming methods, convective forced-air warming is the best in terms of cost, safety, and efficacy.24) Prewarming does not significantly increase core body temperature via thermoregulatory vasodilatation; rather, it increases the heat content of the body, especially in the peripheral thermal compartment.12) In this study, 20 minutes of prewarming using forced air did not alter the tympanic temperature at the end of surgery or affect the incidence of hypothermia. This could be because unlike general or neuraxial anesthesia, the body heat redistribution due to BPB was not significant, even in the control group. Nevertheless, the tympanic temperature in the control group decreased between arrival and discharge from the PACU. This may reflect the effect of exposure to the cold operating room environment, unwarmed intravenous and irrigation fluids, and heat evaporation from surgical incisions rather than an internal core-to-periphery body heat redistribution.2,14) Body heat redistribution caused by general or neuraxial anesthesia manifests as a rapid decrease in core temperature (within 30 minutes to 1 hour after anesthesia induction),6) a phenomenon that was not observed in this study. The perioperative temperature in the prewarming group did not differ significantly from baseline, possibly because prewarming increased the overall heat content of the body.25)
This study has some limitations. First, the core temperature was measured using an infrared thermometer. While infrared thermometers are commonly used in patients receiving regional anesthesia because they are minimally invasive,9,12,19,21) their reliability is controversial.1,26) However, a previous study reported that infrared systems can accurately measure skin temperature as the measurement site (rather than the thermometer used) determines the accuracy and precision of temperature monitoring.14) Another study demonstrated the low bias of an infrared thermometer (IRT 4000; Braun GmbH) to pulmonary artery catheters, suggesting that infrared thermometers could be an alternative for perioperative core temperature measurement.26) Second, the present study excluded patients with a lower preoperative core temperature and pre-existing diseases that could impair thermoregulation. The efficacy of prewarming may differ in patients with various risk factors for postoperative hypothermia. However, further research is required on this topic.
In conclusion, while active prewarming at 43°C for 20 minutes resulted in a lower maximum temperature change than standard preoperative passive insulation, there was no difference in core temperature at the end of surgery. The incidence and severity of perioperative hypothermia, changes in temperature during the perioperative period, thermal comfort scores, and shivering grades were also similar to those of the standard preoperative passive insulation. Therefore, active prewarming may not be routinely required in patients undergoing orthopedic hand surgeries under BPB unless there are multiple risk factors for inadvertent perioperative hypothermia.