



INTRODUCTION
Case 1
Mr. A, a 74-year-old man, presented to the emergency department (ED) with a fever and rigor 2 days after an ultrasound-guided transrectal prostate biopsy. He had a history of benign prostate hypertrophy, stage 2 chronic renal failure, hypertension, and hyperlipidemia and was an ex-smoker of 60 pack-years. He was hypotensive and had generalized tonic-clonic seizures at arrival. He was admitted to the intensive care unit (ICU) for septic shock and was treated with intravenous broad-spectrum antibiotics, inotropic support, and anti-epileptic drugs. His ICU admission was complicated by worsening type 1 respiratory failure due to hospital-acquired pneumonia (HAP). Recurrent failed extubation resulted in a tracheostomy 2 weeks later and 1 month after intubation, before he was successfully weaned off ventilatory support. He was transferred out of the ICU after 5 weeks to a medical ward fully dependent on nasogastric feeding. The geriatric medical team engaged allied health professionals for his care, including physiotherapy, occupational therapy, dietitian, and speech-language therapy. Despite fatigue initially limiting his participation in rehabilitation and complications from HAP and upper gastrointestinal bleeding, he gradually showed improvement under the individualized graded exercise program. On discharge after 4 months in hospital, the patient was able to mobilise with a zimmer frame. Within 1 year, tracheostomy decannulation was performed and the patient returned to normal oral feeding, and in 18 months, the patient fully recovered to independence in all activities of daily living (ADLs).
Three years later, the patient presented to the Geriatrics Clinic for auditory and visual hallucinations, insomnia, and nocturnal wandering. He self-reported cognitive decline, particularly short-term memory loss and word-finding difficulty. His family noted increasing agitation and irritability, as well as increasing difficulties using a cellphone and performing prayers. He denied having depression or anxiety. His wife complained of increased stress because of his behavioral changes, in addition to sleep deprivation and disruption of her daily routine. His Montreal Cognitive Assessment (MoCA) score was 7/20, with memory deficits, delayed recall, language, abstraction, naming, visuospatial, and executive function. He was diagnosed as having moderate-to-severe dementia with behavioral and psychological symptoms of dementia and post-intensive care syndrome (PICS).
Case 2
Ms. T, a 70-year-old woman, presented to the ED with a 4-day history of fever and cough. She had a history of hypertension, hyperlipidemia, and uncomplicated type 2 diabetes mellitus. She was hypoxic and hypotensive despite initial fluid resuscitation and non-invasive ventilatory support. She was admitted to the ICU for severe community-acquired pneumonia, rapid atrial fibrillation, and multi-organ failure. She required short-term hemodialysis for renal support and prolonged intravenous antibiotics for ongoing bacteremia. She underwent a tracheostomy owing to her prolonged need for ventilatory support and nasogastric feeding. After 2 months in the ICU, she was transferred to a geriatric medicine ward and was fully dependent for all ADLs. Her rehabilitation was complicated by fatigue, anxiety, and labile glycemic control. She was discharged after 3 months of hospitalization and was able to transfer to a wheelchair with assistance. Tracheostomy decannulation, normal oral diet, and return to independent mobility were achieved within 1 year. During the clinical follow-up, she reported having anxiety, with occasional flashbacks of her ICU admission. Three years later, she reported having short-term memory loss, which did not affect her ADLs. The patient was diagnosed as having mild cognitive impairment and PICS.
Background
Although survival rates in patients with critical illness and requiring ICU care are increasing, survivors may develop long-term impairments within one or more of the cognitive, psychiatric, and physical domains.1) This cluster of impairments is known as PICS. This diagnosis excludes patients having traumatic brain injuries or stroke. Similar debilitating effects on family members, particularly psychological symptoms among those caring for the patient in the ICU and after discharge, are termed post-intensive care syndrome-family (PICS-F).
It is important to be aware of this condition in older patients. The number of older people with critical illnesses is increasing with an increase in the aging population. Compared with other patient populations, older patients account for more ICU admissions and have a high risk of delirium, which is a risk factor for developing cognitive dysfunction in PICS.2,3)
Approximately 50%–70% of all ICU survivors have at least one PICS-related impairment, which can persist for up to 15 years after discharge.4) A study of Medicare beneficiaries (mean age of 76.9 years) found that 60% of 1,520 ICU hospitalizations with severe sepsis were associated with worsening cognitive or physical functioning 1 year after hospitalization, with 16.7% of survivors showing moderate-to-severe cognitive impairment.5,6) A retrospective cohort study of 21,520 Medicare patients revealed that ICU stays of 3 days or longer, sepsis severity, older age, frailty, depression, and dementia increased the odds of physical disability in older adults receiving home care.7) Another study reported that 15% of older ICU survivors had a new diagnosis of dementia 3 years post-ICU stay, with almost 40% of new dementia cases diagnosed during the first year post-ICU stay.8)
RISK FACTORS FOR PICS
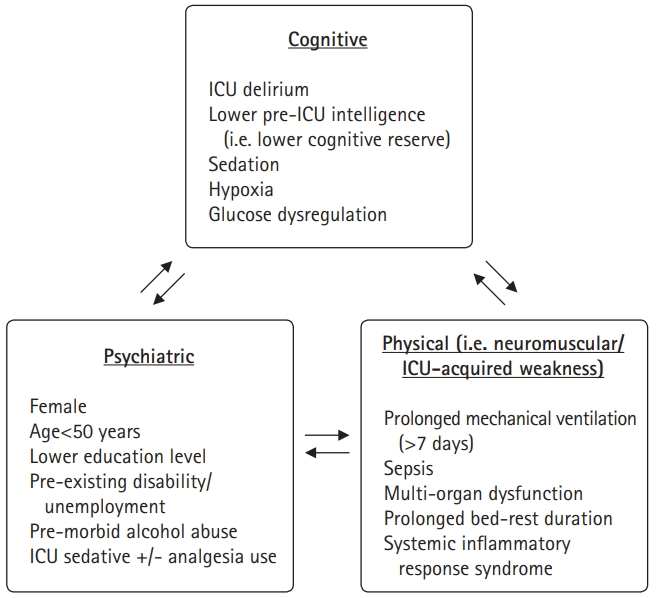
The risk factors for PICS partly depend on which among the cognitive, psychiatric, and physical domains are most affected. These three components are interrelated, with impairment in one domain frequently being associated with worsening function in another. The risk factors for each domain are summarized in Fig. 1.
Cognitive PICS (Case 1)
The major risk factors for cognitive PICS include delirium, poor cognitive reserve, sepsis, and acute respiratory distress syndrome. The duration of delirium is reportedly an independent risk factor for cognitive impairment at 6 and 12 months.9) However, there is no strong evidence suggesting that older adults are at a higher risk for cognitive PICS than are younger adults. A prospective study of 821 ICU patients showed similar cognitive and executive function scores between patients aged 65 years and older and younger patients at 3 and 12 months after discharge.2) Patients with a higher level of education, an indicator of cognitive reserve, had a lower risk of this complication at 3 and 12 months.10) Severe sepsis survivors were three times more likely to develop moderate-to-severe cognitive dysfunction. It is unclear whether cognitive dysfunction is due to acute respiratory distress syndrome itself, complications from sepsis, or the use of mechanical ventilation.
The main cognitive functions affected include attention or concentration, mental processing speed, memory, and executive function. The latter two are necessary for engaging in purposeful, goal-directed behaviors. Loss of these functions tends to impair rehabilitation participation, resulting in poor functional outcomes. Survivors have self-reported severe cognitive impairment after ICU discharge that has persisted for up to 2 years.11)
Physical PICS (Cases 1 and 2)
Approximately 50% of older ICU survivors show functional recovery after critical illness, with a median recovery time of 3 months.6) Older survivors of severe sepsis developed 1.5 new limitations in ADLs, compared with 0.5 in their non-ICU counterparts.12) Older survivors who were mechanically ventilated were 30% more likely to have an ADL disability.13) The physical impairments result in a need for increased support after hospital discharge.
Pre-existing functional disability, cognitive impairment, and frailty are strongly associated with physical PICS or ICU-acquired weakness (ICU-AW). Prolonged mechanical ventilation (>7 days), immobility, ongoing inflammatory response syndrome from sepsis, and multi-organ dysfunction are also associated with the development of ICU-AW. The pathophysiology of this condition is as follows: microvascular ischemia, catabolism, and prolonged immobility cause skeletal muscle wasting, whereas microvascular injury results in nerve ischemia, nerve-related sodium channel dysfunction, and mitochondrial injury. This leads to critical illness-related neuropathy, myopathy, or both.14)
The BRAIN-ICU study found that physical disability significantly contributed to poor mental health and quality of life at 3 and 12 months post discharge.15) However, the nature of this interaction among physical impairment, mental health, and quality of life in ICU survivors requires further evaluation.
Psychiatric PICS (Case 2)
Patients who develop critical illnesses have higher incidences of premorbid psychiatric illness than do patients who do not require ICU hospitalization and the general population.16) Whereas ICU survivors have a 4- to 6-fold higher rate of psychiatric comorbidities than in the general population, those with psychiatric PICS tend to have underlying pre-existing psychiatric disorders. Depression, anxiety, and post-traumatic stress disorder (PTSD) are the three common manifestations of psychiatric PICS, occurring in 19%–37%, 32%–40%, and 19%–22% of patients, respectively.6)
DIAGNOSTIC EVALUATION OF PICS
Diagnosing PICS is challenging because of the failure of early recognition and lack of screening tools for these patients. Serial assessments using history, physical examination, investigations (if required), and multidisciplinary consultations between specialists and therapists are essential to systematically evaluate the PICS domains.
There are no validated cognitive screening tools for PICS. While the MoCA, Mini-Mental State Examination, and Mini-Cog are widely used, they are poor predictors of cognitive impairment at 6 months or longer after discharge.17) As executive dysfunction is the main cognitive domain affected in PICS, the Society of Critical Care Medicine (SCCM) recommends using the MoCA, as it has a component on executive function and is sensitive for detecting mild cognitive impairment.18)
Clinicians should also screen for mood disorders, particularly anxiety, depression, and PTSD.19) Again, there are no adequately validated questionnaires for survivors of critical illnesses. The commonly used tools include the Hospital Anxiety and Depression Scale (HADS), Impact of Events Scale-Revised (IES-R), and the six-item Impact of Event Scale-6 (IES-6). If a mood disorder is identified, patients should be asked about sexual health problems and sleep hygiene, as both issues tend to occur concurrently and may worsen psychiatric PICS.
The manifestations of physical PICS (ICU-AW) can range from generalized poor mobility and multiple falls to generalized muscular weakness. This can be due to disuse or deconditioning; however, definitive diagnoses should be sought for critical illness myopathy (CIM), critical illness polyneuropathy (CIP), and critical illness polyneuromyopathy (CIPNM). CIM tends to be more proximal than distal weakness with sensory preservation and atrophy depending on the illness duration, whereas CIP is more distal than proximal, with limited atrophy. CIPNM is a combination of proximal and distal weaknesses, with distal sensory loss and variable atrophy. For all three types, reflexes tend to be preserved initially but gradually disappear as the weakness progresses, sparing the bulbar musculature.20)
It may be challenging to specify the diagnosis of physical PICS because of the overlap of the conditions and the limited clinical examination possible for sedated or intubated patients. For example, it may be difficult to differentiate between CIP in patients with pre-existing diabetic peripheral neuropathy before ICU admission. However, as with both patients described here, failure to wean off ventilatory support may be an early indicator of physical PICS, requiring confirmatory electrodiagnostic tests such as nerve conduction studies and electromyography.
One of the main tests used to measure changes in strength and functional outcomes in the ICU is the physical function outcome measure (PFIT). This tool was initially developed to measure endurance, strength, cardiovascular capacity, and functional level among mechanically ventilated tracheostomy patients who were able to stand, with the test repeated after weaning from ventilation.21) The tests involved assessments of strength for shoulder flexion and knee extension, level of assistance required for sit-to-stand, and step cadence in steps per minute. The PFIT demonstrated high inter-rater reliability and sensitivity in ICU patients.22)
In the ICU setting, the 6-minute walk test (6MWT) and Timed Up and Go (TUG) test may not be practical, as they require space and consideration of how to manage drips, drains, and oxygen delivery systems when the patient is walking or turning. However, a 6MWT should be performed in extubated and mobile ICU patients. A randomized controlled trial of patients admitted to the ICU for 5 days or longer comparing the results of the 6MWT, TUG, and PFIT at admission, discharge, and follow-up showed that the 6MWT was able to demonstrate the rate of change over time and between-group differences for the intervention group (intensive exercises in ICU, wards, and outpatients) and the control group (standard care).23) Thus, for ICU patients, although the PFIT may be used for initial assessment, the 6MWT should be used for follow-up once the patient is extubated and able to start mobilizing.
It is important to obtain early input from physiotherapists and occupational therapists for assessment and management, including preemptive prevention of complications such as contractures, preferably while the patient is still in the ICU.20,24) Comprehensive geriatric assessment should be performed, with continual assessment and rehabilitation until discharge. Dietitian input for nutrition assessment and intervention is important to ensure that nutritional requirements are met during the recovery phase.
It is also crucial to identify the presence and severity of pre-existing illnesses within the three domains, as unchanged symptoms do not support the diagnosis of PICS. This is challenging for those without the cognitive capacity to compare their current status with symptoms before admission. Engagement with close family members is beneficial in identifying the presence and nature of pre-existing comorbidities. In addition to collateral history obtained from caregivers and family, pre-existing clinical records of diagnoses, investigations, cognitive tests, and functional assessments, such as from previous physiotherapy sessions (if available), are valuable in objectively confirming acute changes post-ICU stay compared with baseline. Unfortunately, the cognitive status before ICU admission, particularly objective measures, is usually unavailable. A systematic review also found that most publications on PICS lacked information on baseline cognitive status; thus, it was not possible to determine whether the observed cognitive deficits arose de novo or represented worsening of pre-existing cognitive deficits.25)
MANAGEMENT OF PICS
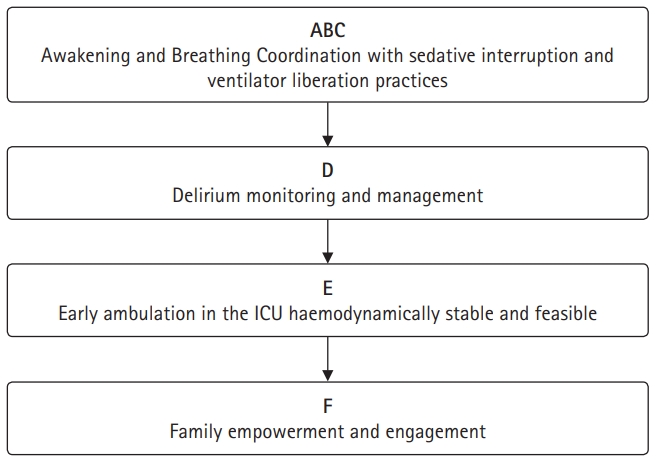
The management of PICS is divided into two parts: within the ICU and post-ICU stay. Intensivists can reduce the risk of PICS by minimizing sedation, avoiding psychotropic use including antipsychotics and anticholinergic agents, avoiding hypoglycemia and hypoxemia, environmental modifications, and prioritizing early physical rehabilitation and mobility for older people. The ABCDEF bundle approach shown in Fig. 2 has been shown to reduce the likelihood of death within 7 days, mechanical ventilation, coma, delirium, and the use of physical restraints.26,27)
Treatment of patients with PICS involves managing individual impairments in each domain through multidisciplinary care. The physician responsible should coordinate care with other clinicians and allied health professionals. Early physical therapy once a patient is stable from cardiorespiratory and neurological perspectives may decrease cognitive impairment, improve physical function, and reduce psychiatric comorbidity. Cognitive enhancers and cognitive rehabilitation through memory training are not effective in PICS. Thus, further studies are needed to identify evidence-based treatments for this condition.
Although there is limited evidence to guide the discontinuation of antipsychotics in the post-ICU phase, it is recommended to use the smallest dose possible for behavioral disturbance from postoperative delirium and to discontinue their administration as soon as possible.16) If antipsychotics are required after discharge, the benefits versus risks should be considered for individual patients.
The optimal follow-up and natural progression of PICS remain uncertain, but most patients are followed up for several years at regular intervals. We recommend follow-ups every 3 months after discharge, followed by individualized intervals according to the needs of each patient. This is important, as symptoms may become more apparent at a later stage, as seen in Case 1. The care of older people with PICS requires a multidisciplinary approach, including intervention by medical specialists, general practitioners, therapists, and social services. If available, referrals to established PICS peer support groups may assist in reducing psychological stress. Although PICS clinics have been introduced in the UK and the United States, evidence of their benefits remains conflicting.
The symptoms and signs of PICS improve modestly over the first 6 to 12 months after ICU discharge. However, most patients have deficits persisting for years, with an associated inability to work, a reduced quality of life, and an increased risk of mortality.28) The effects of preventative or therapeutic interventions on these outcomes remain unknown, as is the risk for subsequent hospitalizations, critical illnesses, or PICS recurrence.
An important component of the ABCDEF bundle is family empowerment and engagement. Clinicians should evaluate family members for PICS-F, as they may also develop persistent physical and psychological symptoms after patient discharge. The risk factors for PICS-F are divided into those related to caregivers, patients, and the healthcare system. Caregiver factors associated with the development of PICS-F include female sex, spouse caregiver, low education level, pre-existing mental or physical illness, family history of mental illness, lack of social and professional support, and caregiving for more than 100 hours per month.29) Healthcare-system or ICU-related factors are potentially modifiable, such as limited ICU visiting hours, patient perception of being near death, and communication skills of ICU physicians. Patient-related factors play only a small role in the development of PICS-F, according to the findings of the RECOVER study.30)
The SCCM recommends family involvement in the care of ICU patients. However, these guidelines lack recommendations on how and when to screen family members and who is responsible for assessing and managing PICS-F. Although further research is required to validate screening tools for PICS-F, we recommend close monitoring of family member well-being and considering referral for psychotherapy if indicated.
Studies have shown that the following approaches are useful to improve both patient and family outcomes, resulting in a high level of family satisfaction and reduced family anxiety: creation of “open” ICUs, family witness of resuscitation efforts, ICU diaries, and proactive engagement of family members in patient care.31,32) “Open” ICUs are characterized by flexible visiting policies in terms of hours, number or age of visitors, daily meetings with family members, healthcare providers performing tasks in front of family members, and redesigning units to ensure family comfort and sleep needs. Incorporating family members into ICU care and witnessing codes have been shown to reduce depression and PTSD risk at 3 and 12 months post discharge.33) Most studies support the use of ICU diaries to document events chronologically, with entries from staff and family members and photographs of patients.34)
Effective, structured communication strategies between staff and family members are also useful in reducing the risk of developing PICS-F. Useful approaches include conducting a family conference within 72 hours of ICU admission, ensuring consistent communication from different team members, and increasing the proportion of time spent listening rather than talking. Empathy is required to recognize the difficulties of being a surrogate decision-maker and having a critically ill or experiencing the impending loss of a loved one. Clinicians should identify opportunities to acknowledge and address family emotions, explore patient values and treatment preferences, explain the role of surrogate decision-makers, and affirm non-abandonment of the patient and family, even if the patient is dying.35) These principles are summarized in the mnemonic “VALUE” (Value family statements, Acknowledge and Listen to family emotions, Understand patients as persons, and Elicit family questions) and have been shown to reduce PICS-F symptoms and increase family confidence in the care team.36,37)
Evidence is limited or lacking regarding specific post-ICU interventions to reduce symptoms of PICS or PICS-F.38) A major barrier to conducting large-scale, multi-site studies is the variability of post-ICU follow-up. Patients and caregivers, particularly in rural and underserved areas, may receive follow-up at different hospitals or healthcare systems from their initial ICU admission. In addition to rehabilitation and follow-up, we recommend that patients and caregivers be provided access to support services such as home health care and the integration of care with the involvement of primary care physicians before discharge.
Whereas post-ICU clinics can provide interventions for the management of PICS-F, family-centered care remains inconsistent, with ambiguity in which healthcare professionals are responsible for managing PICS-F. This is a significant issue, as the effects of PICS-F may be long-lasting and profoundly impact caregivers’ quality of life.
Meanwhile, clinical practice guidelines and protocols are needed for the diagnosis and management of the physical and neuropsychiatric sequelae of PICS. These interventions should be system-based yet individualized to each ICU survivor and developed through collaboration among intensivists, geriatricians, and multidisciplinary teams. A recovery care coordinator should also be designated to enable care coordination for the patient and caregivers from the ICU, as well as the implementation of individual care plans to facilitate a smooth transition of care from ICU to outpatient settings.2)
Once there is improved recognition and identification of PICS, further research is needed to create an evidence-based approach and model of care to effectively manage this condition. More research is also required to elucidate the mechanism for each component of PICS (cognitive, physical, and psychiatric), develop sensitive screening tools and specific confirmatory tests, and evaluate the effectiveness of preventive and treatment approaches for this condition.
CONCLUSION
There is limited awareness and under-recognition of PICS among clinicians despite its significant impact on the function and quality of life of patients and families. This condition may be prevented by encouraging early mobility in the ICU and minimizing the use of sedatives and antipsychotics. Once PICS is identified, rehabilitation, management, and follow-up should be carried out by a multidisciplinary team. Further research is required to strengthen the evidence base for the diagnosis and management of PICS and PICS-F.